
BTK inhibitors and drug desensitization are emerging areas of allergy research. Investigators are exploring whether BTK inhibitors can reduce immediate hypersensitivity reactions during high-risk drug administration.
Educational Content Disclaimer: This article is for educational purposes only. It is not medical advice and should not replace consultation with a qualified allergist or specialist. The concepts discussed are investigational, hypothesis-generating, and not approved for routine clinical use. This post is intended as a specialist perspective piece, not a practice recommendation.
Some patients face a difficult dilemma: they need a medication that could save their life — a platinum-based chemotherapy, a biologic, or even insulin — but they have developed a dangerous allergic reaction to it. Drug desensitization has become one of the most important tools for managing this situation. Yet even with careful protocols, breakthrough reactions still occur, and some patients remain at high risk.
What if we could temporarily suppress the allergic signaling pathway itself during drug administration? A growing body of mechanistic and early clinical evidence is beginning to make this idea more than theoretical.
🔬 What Is BTK and Why Does It Matter in Allergy?
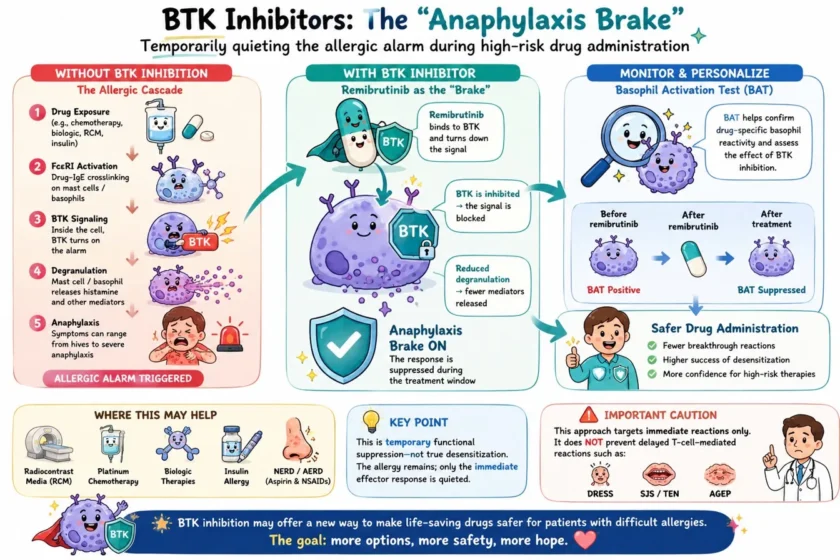
Bruton’s tyrosine kinase (BTK) is an intracellular signaling enzyme that plays a central role in activating mast cells and basophils — the immune cells responsible for immediate allergic reactions including anaphylaxis.
In a classic IgE-mediated allergic reaction, the sequence runs:
FcεRI activation → BTK signaling → Mast cell / basophil degranulation → Histamine release → Anaphylaxis
When BTK is inhibited, mast cells and basophils become significantly less able to release histamine and other inflammatory mediators. BTK inhibition is believed to contribute substantially to the clinical efficacy of remibrutinib (Rhapsido®) — recently FDA-approved for chronic spontaneous urticaria (approved September 2025) — by reducing mast-cell and basophil activation, though the full pathophysiology of CSU involves additional autoallergic and autoimmune contributors.
The critical difference from biologics like omalizumab is speed. Omalizumab requires weeks to meaningfully lower free IgE levels. Studies suggest that BTK inhibitors can achieve significant BTK occupancy and basophil suppression within hours of dosing, raising the possibility of using a short-course regimen as a “functional shield” before high-risk drug administration.
💊 BTK Inhibitors and Drug Desensitization: How Could They Work?
Rapid drug desensitization (RDD) works by gradually exposing a patient to increasing doses of a drug to induce temporary tolerance. It is highly effective in many situations but has real limitations — some patients experience breakthrough reactions despite careful protocols, requiring emergency treatment or even abandonment of the procedure.
A short course of a BTK inhibitor before RDD could theoretically:
- Reduce mast-cell and basophil activation during dose escalation
- Suppress breakthrough anaphylaxis
- Improve procedure completion rates
- Potentially simplify multi-step protocols
The concept of short-course BTK inhibitor pretreatment before high-risk drug administration is currently a research hypothesis. No validated pretreatment protocol exists, and optimal agent selection, dosing, and timing remain to be established in prospective studies.
🧪 Clinical Evidence for BTK Inhibitors and Drug Desensitization
This concept is not purely theoretical. Early case reports have already demonstrated that BTK inhibitors can facilitate difficult desensitization procedures.
A published case report describes the successful use of ibrutinib to prevent severe breakthrough reactions during rapid drug desensitization to brentuximab vedotin and gemcitabine chemoimmunotherapy in a patient with refractory Hodgkin’s lymphoma who had experienced severe anaphylaxis requiring epinephrine during a prior treatment cycle. More recently, acalabrutinib has also been explored as an adjunct strategy in platinum-based chemotherapy desensitization.
At present, published evidence consists primarily of isolated case reports and small proof-of-concept experiences rather than controlled clinical trials. These reports involve only small numbers of patients, but they provide important early proof-of-concept that transient BTK inhibition can suppress immediate hypersensitivity reactions sufficiently to improve the safety of high-risk drug administration.
Remibrutinib possesses pharmacologic characteristics — high BTK selectivity, rapid onset, oral administration, and a more favorable off-target safety profile than older agents — that make it an attractive candidate for future investigation in this setting. However, published desensitization experience to date involves primarily ibrutinib, and whether remibrutinib offers clinical advantages in this specific context remains to be demonstrated.
🧲 Beyond Facilitation: Could BTK Inhibitors Temporarily Suppress Effector Pathways During Drug Exposure?
A more provocative concept goes further than merely assisting desensitization. Short-course BTK inhibition might suppress mast-cell and basophil degranulation sufficiently to markedly attenuate immediate effector-cell activation in selected contexts during a defined drug exposure window.
In this model, a BTK inhibitor would function less as a desensitizing agent and more as a temporary “anaphylaxis brake” — achieving transient effector-pathway suppression while the drug is active. Importantly, this would not mean the patient is no longer allergic. The underlying sensitization would remain; only the immediate effector response would be transiently suppressed.
This concept would still require carefully supervised graded exposure and specialist oversight, because complete suppression of tissue mast cells cannot be guaranteed, and some reactions may involve BTK-independent mechanisms such as complement activation, MRGPRX2-mediated pseudoallergy, or cytokine-release pathways.
🩸 Could Basophil Activation Testing Help Guide BTK-Assisted Drug Administration?
An intriguing translational question is whether the basophil activation test (BAT) could serve as a functional pharmacodynamic biomarker in this setting. In principle, baseline BAT could confirm drug-specific basophil reactivity before the procedure, while a repeat BAT after BTK inhibitor pretreatment could objectively demonstrate the degree of pharmacological suppression achieved. If residual BAT reactivity correlates with breakthrough reactions during subsequent drug exposure, this would provide a practical tool for individualized risk stratification — helping identify which patients are sufficiently protected to proceed and which may require additional precautions.
This remains a research hypothesis. Future translational studies will be needed to determine whether BTK inhibitor-induced BAT suppression reliably predicts clinical protection during drug administration.
🏥 Potential Applications of BTK Inhibitors and Drug Desensitization
An important overarching consideration applies across all scenarios below: many reactions currently managed with rapid drug desensitization — including platinum, taxane, and monoclonal antibody reactions — involve mixed or non-IgE mechanisms, including IgG-mediated complement activation, cytokine release, and direct mast-cell activation. The relative benefit of BTK inhibition is therefore likely to vary across drug classes and reaction endotypes, with the greatest effect expected in reactions predominantly driven by FcεRI-mediated mast-cell and basophil activation.
Radiocontrast Media (RCM) Reactions
Contrast media reactions present a unique challenge: large volumes must be administered rapidly, procedures are often urgent, and conventional slow desensitization protocols may not accurately reflect real-world contrast exposure conditions.
An important mechanistic caveat applies here: true IgE-mediated allergy to modern non-ionic radiocontrast media is uncommon. Most contrast reactions represent direct, non-IgE-mediated mast cell and basophil activation — likely through MRGPRX2 or osmotic mechanisms — that may be partially or entirely BTK-independent. Whether BTK inhibition meaningfully suppresses these pseudoallergic pathways remains an open question, and the rationale for its use in RCM reactions is therefore less certain than for confirmed IgE-mediated drug allergy.
Insulin Allergy
Insulin desensitization creates an inherent paradox: the drug being desensitized can itself cause hypoglycaemia during very slow escalation protocols. BTK inhibition might theoretically allow safer reintroduction of therapeutic insulin doses while limiting allergic reactions, without requiring prolonged low-dose escalation protocols.
Chemotherapy and Biologic Reactions
Breakthrough reactions continue to occur during desensitization to platinum agents, taxanes, and monoclonal antibodies. Short-course BTK inhibition could potentially improve the safety margin of rapid desensitization strategies and reduce the need for emergency intervention. However, as noted above, reactions to these agents frequently involve mechanisms beyond FcεRI/BTK — including IgG, complement, and cytokine pathways — and the degree of benefit from BTK inhibition may be partial or variable depending on the dominant reaction endotype.
Aspirin Desensitization in NSAID-Exacerbated Respiratory Disease (NERD)
Mast cells contribute to airway inflammation in NERD, and BTK inhibition might reduce reaction severity during aspirin challenge. However, the mechanistic limitations here are substantial.
Aspirin-induced reactions in NERD are driven primarily through COX-1 inhibition, with downstream overproduction of cysteinyl leukotrienes and thromboxane rather than IgE-mediated mast cell activation. The core pathophysiology therefore operates largely upstream of BTK-dependent signalling. BTK inhibition might dampen overall mast cell reactivity at the margins, but it is unlikely to address the fundamental prostaglandin-leukotriene imbalance that underlies both the reaction and the development of true aspirin tolerance. Whether suppression of symptoms during the procedure would allow genuine desensitisation to proceed normally, or simply mask the reaction without permitting the necessary biochemical shift, remains an important unanswered question.

⚠️ Important Concerns and Limitations
Does this produce true desensitization?
Traditional RDD induces genuine temporary immunological tolerance through receptor anergy and mediator depletion. BTK inhibition may instead pharmacologically mask reactions while the patient remains fundamentally sensitized. If so, tolerance could disappear rapidly after stopping the drug, and subsequent unprotected exposure could still trigger anaphylaxis. This distinction between pharmacologic suppression and true immunological tolerance is critical and must not be conflated.
What about delayed reactions?
BTK inhibition acts selectively on mast cells and basophils within the immediate allergic effector pathway. It has no meaningful effect on CD8+ cytotoxic T-cell responses, which drive the most severe delayed drug reactions through granulysin and perforin-mediated keratinocyte destruction. DRESS, Stevens-Johnson syndrome, TEN, and AGEP are fundamentally T-cell-mediated conditions — BTK inhibition is mechanistically irrelevant to their prevention, and clinicians must understand that suppression of an immediate reaction provides no protection whatsoever against these life-threatening delayed syndromes.
Could severe reactions still occur?
Even with BTK inhibition, tissue mast cells may not be completely suppressed. Some immediate reactions involve BTK-independent mechanisms. Supervised monitoring remains essential regardless.
Safety profile of BTK inhibitors
First-generation BTK inhibitors such as ibrutinib carry significant adverse effects relevant to short-term use, including bleeding risk, cardiac arrhythmias, and immunosuppression. Remibrutinib, being highly selective, appears more favourable in this regard, but safety data specifically in the desensitization context do not yet exist for any BTK inhibitor.
🔑 Key Takeaways
|✅|BTK inhibitors suppress mast-cell and basophil activation — a key effector pathway in many forms of immediate hypersensitivity and anaphylaxis |
|🧪|Early case reports (primarily with ibrutinib) support BTK inhibitor-assisted desensitization as proof-of-concept |
|💊|Remibrutinib acts within hours — unlike omalizumab, which requires weeks — but clinical desensitization data for remibrutinib specifically are lacking|
|🩸|BAT suppression may emerge as a translational pharmacodynamic biomarker — currently a research hypothesis |
|⚠️|Evidence remains limited to isolated case reports — no validated protocol or controlled trial exists |
|🔀|Benefit likely varies by reaction endotype — greatest for FcεRI-driven reactions, less certain for mixed or non-IgE mechanisms |
|❌|BTK inhibition does not prevent CD8+ T-cell-mediated reactions — DRESS, SJS/TEN, and AGEP remain possible |
|🔍|RCM and NERD rationale is mechanistically weaker — most reactions in these settings are not primarily BTK-dependent |
|👨⚕️|Any off-label use should only be considered within a research setting or under specialist supervision with careful monitoring |
Whether BTK inhibitors ultimately prove most useful as adjuncts to conventional rapid drug desensitization or as stand-alone pharmacologic protection strategies during high-risk drug exposure remains unknown — but the concept may open an entirely new direction in translational allergy research.
📚 References
- Rodsaward P, et al. Pretreatment with ibrutinib facilitates rapid drug desensitization in a difficult case of brentuximab vedotin-induced anaphylaxis. J Allergy Clin Immunol Pract. 2023;11(2):642–4.
- Lin, E. V., Suresh, R. V., & Dispenza, M. C. (2024). Bruton’s tyrosine kinase inhibition for the treatment of allergic disorders. Annals of Allergy, Asthma & Immunology, 133(1), 33-42.
- Smiljkovic, D, et al. BTK inhibition is a potent approach to block IgE‐mediated histamine release in human basophils. Allergy, 2017, 72.11: 1666-1676.
- Novartis. FDA approves Rhapsido (remibrutinib) for chronic spontaneous urticaria. September 30, 2025.